
History:
A 47-year-old woman presented with chronic mid-back pain, along with bilateral lower limb radiculopathy. These symptoms had been troubling her for several months and were clinically indicative of a lumbar spinal infection or spine infection due to tuberculosis.
She suffered from neurogenic claudication, limiting her walking ability to just 10–15 minutes. The pain worsened while rising from a seated position, and she often required support for balance—signs often seen in patients with an infected spine or spinal instability caused by vertebral infection.
Her gait pattern showed forward stooping, and she was unable to perform toe or heel walking, suggesting neurological weakness linked to the spinal infection.
She also reported sleep disturbances due to persistent spinal discomfort. Notably, she had a history of pulmonary tuberculosis in 1998 and had received anti-tubercular treatment (ATT) for two months—making spinal tuberculosis (Pott’s disease) a likely cause of the current lumbar spinal infection.
Surgical Management:
To treat the advanced case of dorsal spine tuberculosis (Pott’s spine), the patient underwent D9-D10 spinal debridement and decompression, followed by posterior spinal fusion from D7 to L1. This surgical procedure was performed to effectively remove infected spinal tissue, relieve pressure on the spinal cord, and restore spinal stability. The long-segment fusion helped prevent kyphotic spinal deformity and maintain proper alignment, promoting better recovery and long-term spine health.
On Clinical Examination:
During physical examination, the patient exhibited localized tenderness over the dorsal spine, especially around the T9 vertebral level, strongly suggesting inflammatory spine infection or tuberculous spondylodiscitis.
Right Extensor Hallucis Longus (EHL): 4/5
Bilateral Hip Flexors: 3/5
Despite the weakness, sensory and reflex exams were normal, indicating that the lumbar spine infection had not caused widespread neurological compromise. Peripheral circulation was intact in all limbs.
Radiological and Laboratory Investigations:
MRI Spine:
MRI findings were consistent with tubercular spine infection involving the lumbar and dorsal segments:
- Lytic destruction of D8–D9 vertebral endplates and disc space.
- A large pre/paravertebral and epidural abscess from T7 to T11.
- Severe spinal cord compression at T9.
- Spinal canal stenosis at T9–T10 with canal diameter of 0.5 cm
These findings were typical of vertebral osteomyelitis caused by spinal tuberculosis, also termed Pott’s spine.
GeneXpert Test (disc sample):
Detected Mycobacterium tuberculosis, confirming spinal TB infection
Histopathology Report:
Showed granulomatous inflammation, confirming tuberculous vertebral infection.
Sputum Gram Stain:
Revealed gram-positive cocci, suggesting a possible secondary bacterial spine infection.
Before Surgery

Surgical Management:
Given the severity of the lumbar spinal infection, the patient underwent surgery which included:
- D9–D10 spinal debridement and decompression
- Posterior spinal instrumentation and long-segment fusion from D7 to L1.
The aim was to:
- Remove infected spinal tissues.
- Relieve pressure on the spinal cord.
- Prevent kyphotic deformity.
- Restore alignment and stability to the infected lumbar spine
The surgery used Kentro implants under general anesthesia and provided strong mechanical support for the spine damaged by infection.
After Surgery
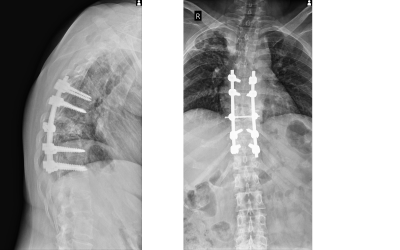
Post-Surgical Care and Discharge Status:
After surgery, the patient was started on the HRZE regimen (first-line anti-tubercular therapy), combined with supportive medications.
She showed excellent recovery:
- Ambulated with full weight-bearing using a walker.
- Climbed stairs with assistance.
- No fever or wound complications.
- Clean and dry Tegaderm dressing.
She was discharged in a stable clinical condition with advice for regular follow-ups and medication adherence.
Long-Term Prognosis and Recovery:
With early diagnosis, timely surgical intervention, and ongoing ATT, the prognosis for this patient with a lumbar spinal infection is highly favorable.
Expected outcomes include:
- Resolution of tuberculous spine infection.
- Restoration of spinal stability and alignment
- Relief from radicular pain
- Return to independent daily activities.
Regular monitoring and strict compliance with anti-tubercular medication will help ensure full recovery from this serious spinal infection and prevent recurrence.